The Hidden Cost of Modern Work
As a neurosurgeon, one of the most common complaints I hear from IT professionals is:
“Doctor, I have neck pain.”
Some describe a dull ache at the base of the neck. Others complain of stiffness, headaches, shoulder pain, tingling in the hands, or pain radiating down the arm. A few eventually develop cervical disc prolapse, nerve compression, or spinal canal stenosis.
The interesting part is that many of these individuals are young—sometimes in their late twenties or thirties.
The question is simple:
Why are so many IT professionals developing neck pain?
The answer lies not in one single factor but in a combination of posture, prolonged sitting, lifestyle habits, stress, poor sleep, lack of exercise, and continuous exposure to digital devices.
Understanding these factors can help prevent years of discomfort and potentially avoid serious spine problems in the future.
Understanding the Anatomy of the Neck
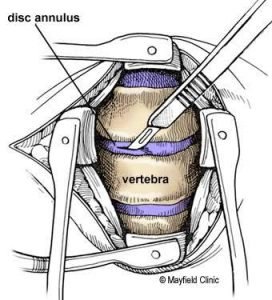
The cervical spine, commonly called the neck, consists of seven vertebrae numbered C1 to C7.
Between these vertebrae are intervertebral discs that act as shock absorbers.
The neck supports the weight of the head, which typically weighs between 4 and 6 kilograms.
In addition to supporting the head, the cervical spine allows us to:
- Look up and down
- Turn left and right
- Tilt the head sideways
- Maintain balance
The neck also protects the spinal cord and the nerves that travel to the shoulders, arms, and hands.
When the neck is positioned correctly, these structures work efficiently.
When poor posture is maintained for hours every day, the load on the spine increases dramatically.
The Problem of Prolonged Sitting
Many IT professionals spend 8 to 12 hours a day sitting in front of a computer.
Some work from offices.
Many work from home.
The human spine was not designed to remain static for such long durations.
Our bodies are designed for movement.
When we sit continuously:
- Neck muscles become fatigued
- Shoulder muscles tighten
- Blood circulation decreases
- Joint mobility reduces
- Spinal discs experience continuous pressure
Over months and years, this repeated stress accumulates and begins to affect the spine.
The body often gives warning signals in the form of:
- Neck pain
- Stiffness
- Headaches
- Muscle spasms
Unfortunately, these early signs are often ignored.
Forward Head Posture: The Silent Enemy
One of the most common postural problems seen in IT professionals is forward head posture.
The head gradually moves in front of the shoulders while working on a laptop, desktop, or mobile phone.
For every inch the head moves forward, the effective load on the neck increases significantly.
A head weighing 5 kilograms may effectively place 15 to 25 kilograms of force on the cervical spine when positioned improperly.
Imagine carrying a heavy weight all day.
That is essentially what many neck muscles experience.
Over time, this leads to:
- Muscle fatigue
- Ligament strain
- Joint stress
- Disc degeneration
This is one of the major reasons why neck pain develops.
Poor Workstation Ergonomics
Many professionals invest heavily in technology but overlook ergonomics.
Common mistakes include:
- Monitor placed too low
- Monitor placed too high
- Chair without lumbar support
- Working from the bed
- Working from the sofa
- Using dining chairs for long hours
- Laptop screens positioned below eye level
When the monitor is not aligned correctly, the neck remains bent for prolonged periods.
Even a slight deviation maintained for hours can create substantial strain.
The ideal monitor position should allow the top of the screen to remain near eye level while maintaining a neutral neck posture.
Working from Sofas and Bean Bags
The work-from-home culture introduced new problems.
Many individuals now work:
- On sofas
- On recliners
- On beds
- On bean bags
While these may appear comfortable initially, they often force the neck into awkward positions.
A twisted or flexed neck maintained for hours places excessive stress on muscles, discs, and joints.
The body can tolerate these positions briefly.
It cannot tolerate them every day for years.
Failure to Take Breaks
The spine thrives on movement.
Yet many IT professionals remain seated for several hours without interruption.
Meetings follow coding sessions.
Coding sessions follow presentations.
Presentations follow emails.
Hours pass without standing up.
A simple five-minute break every hour can significantly reduce strain on the cervical spine.
Standing, stretching, walking, and changing posture allow muscles and joints to recover.
Ignoring breaks allows fatigue to accumulate throughout the day.
Mobile Phones: The Second Work Shift
After completing work on the computer, many individuals transition directly to mobile phones.
They spend additional hours:
- Watching videos
- Browsing social media
- Playing games
- Reading messages
Most of this occurs with the neck bent forward.
This repetitive position creates what is commonly called “text neck.”
Many patients who complain of persistent neck pain spend more time on their phones after work than they spend exercising.
The neck never receives an opportunity to recover.
Sleep: The Forgotten Therapy
Sleep is when the body repairs itself.
Unfortunately, sleep quality has deteriorated in many working professionals.
Common issues include:
- Sleeping late
- Irregular schedules
- Inadequate sleep duration
- Poor mattress quality
- Improper pillow support
Some individuals sleep on unsuitable surfaces.
Others sleep without proper neck support.
The cervical spine requires neutral alignment during sleep.
Poor sleeping posture can aggravate muscle strain and contribute to chronic neck pain.
A good mattress and appropriate pillow are often underestimated but play a significant role in spinal health.
Stress and Neck Pain
Many people view neck pain as purely mechanical.
However, stress plays a major role.
- Deadlines
- Targets
- Meetings
- Performance reviews
- Job uncertainty
- Long working hours
All contribute to muscle tension.
Under stress, muscles around the neck and shoulders tend to tighten.
This sustained tension can lead to:
- Neck stiffness
- Headaches
- Shoulder pain
- Muscle spasms
Stress management is therefore an essential part of neck pain prevention.
The Role of Smoking
Smoking accelerates degeneration of spinal discs.
Nicotine reduces blood supply to tissues.
Discs receive fewer nutrients.
Healing becomes slower.
Degeneration progresses faster.
Studies consistently show that smokers have a higher risk of spinal problems compared to non-smokers.
For professionals already exposed to poor posture and prolonged sitting, smoking further increases the risk.
Energy Drinks and Excessive Coffee
Coffee in moderation is generally acceptable.
However, relying excessively on caffeine and energy drinks to overcome fatigue can create other issues.
Many professionals use caffeine to compensate for:
- Poor sleep
- Excessive workload
- Mental fatigue
This often leads to a cycle of poor recovery and chronic muscle tension.
No energy drink can replace proper sleep, exercise, and recovery.
Poor Nutrition and Musculoskeletal Health
The spine requires proper nutrition.
Many working professionals skip meals or rely heavily on processed foods.
Deficiencies in:
- Protein
- Vitamin D
- Vitamin B12
- Calcium
- Magnesium
can affect muscle health and recovery.
Poor nutrition does not directly cause disc prolapse, but it may contribute to muscle fatigue, reduced healing capacity, and chronic pain.
Online Neck Gadgets: A Word of Caution
Many individuals attempt self-treatment by purchasing gadgets online.
These include:
- Neck traction devices
- Massagers
- Posture correctors
- Neck stretching tools
While some products may provide temporary relief, not every gadget is suitable for every person.
Improper use may worsen symptoms.
Persistent neck pain should be evaluated properly rather than relying solely on online solutions.
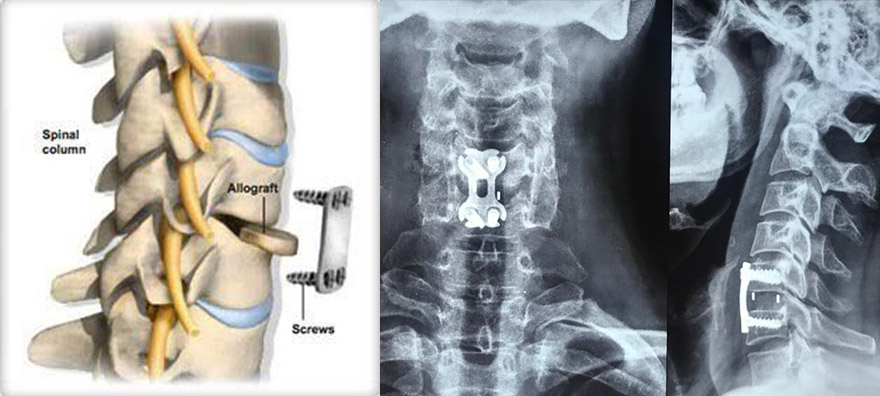
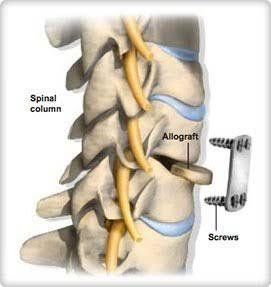
When Neck Pain Progresses to Disc Prolapse
Not all neck pain is dangerous.
However, persistent mechanical stress can contribute to disc degeneration.
As discs age and weaken, they may bulge or prolapse.
A cervical disc prolapse can compress nearby nerves and cause:
- Arm pain
- Numbness
- Tingling
- Weakness
In more severe cases, spinal cord compression may occur.
This condition is known as cervical myelopathy and requires prompt medical evaluation.
Cervical Canal Stenosis
Some individuals gradually develop narrowing of the spinal canal.
This is called cervical canal stenosis.
Symptoms may include:
- Difficulty with balance
- Hand clumsiness
- Numbness
- Weakness
- Walking difficulties
Early recognition is important because prolonged spinal cord compression can lead to permanent neurological deficits.
Does It Affect Men and Women Differently?
Both men and women develop neck pain.
However, patterns may vary.
Men often report symptoms related to prolonged sitting, driving, and extended work hours.
Women frequently balance professional responsibilities with household responsibilities, increasing overall physical and mental stress.
Hormonal factors, muscle mass differences, and ergonomic challenges may also influence symptom patterns.
Ultimately, the fundamental causes remain similar:
- Prolonged static posture
- Inadequate recovery
- Poor spinal habits
How IT Professionals Can Protect Their Neck
Simple steps can make a substantial difference:
- Maintain proper workstation ergonomics.
- Keep the monitor at eye level.
- Use a supportive chair.
- Avoid working from sofas and bean bags.
- Take a five-minute break every hour.
- Perform regular neck and shoulder stretches.
- Limit unnecessary mobile phone use.
- Exercise regularly.
- Maintain healthy body weight.
- Stop smoking.
- Prioritize quality sleep.
- Eat a balanced, nutritious diet.
- Stay hydrated.
- Seek medical advice if symptoms persist.
Final Thoughts
Neck pain among IT professionals is not merely a consequence of aging.
It is often the result of cumulative stress placed on the cervical spine through years of:
- Poor posture
- Prolonged sitting
- Inadequate movement
- Excessive screen time
- Stress
- Poor sleep
- Unhealthy lifestyle habits
The encouraging news is that many of these factors are modifiable.
The goal should not be simply treating neck pain after it develops.
The goal should be preventing it before it affects quality of life, productivity, and long-term spinal health.
Your neck supports your head every minute of every day.
Taking care of it is not a luxury—it is an investment in your future health and wellbeing.
Frequently Asked Questions
1. Why do IT professionals commonly develop neck pain?
IT professionals often spend prolonged hours sitting in front of computers with poor posture, inadequate workstation ergonomics, limited movement, and excessive screen time. Over time, these factors place continuous stress on the cervical spine, muscles, and ligaments, increasing the risk of chronic neck pain and cervical disc problems.
2. Can prolonged computer use cause a cervical disc prolapse?
Prolonged computer use alone does not directly cause a cervical disc prolapse. However, years of poor posture, forward head position, prolonged sitting, lack of exercise, and age-related disc degeneration can contribute to disc bulging or prolapse, especially when combined with other lifestyle factors.
3. What is the best sitting posture to prevent neck pain while working?
Maintain a neutral spine with your ears aligned over your shoulders. Keep the monitor at eye level, shoulders relaxed, elbows at about 90 degrees, feet flat on the floor, and use a chair with good lumbar support. Avoid leaning forward or looking down at the screen for prolonged periods.
4. How often should I take breaks while working on a computer?
A good practice is to stand up and move every 45–60 minutes. Take a 5-minute break to walk, stretch your neck, shoulders, and back, and allow your muscles to relax. Regular movement helps reduce muscle fatigue and improves circulation.
5. When should neck pain be evaluated by a neurosurgeon or spine specialist?
Seek medical evaluation if your neck pain persists for more than a few weeks despite rest, or if it is associated with arm pain, numbness, tingling, weakness, difficulty using your hands, balance problems, or bowel/bladder symptoms. Early assessment can help identify conditions such as cervical disc prolapse or spinal canal stenosis before they progress.
6. Can neck pain in IT professionals be prevented?
Yes. Most work-related neck pain can be reduced by maintaining proper ergonomics, taking regular movement breaks, performing neck and shoulder strengthening exercises, sleeping on a supportive mattress and pillow, limiting excessive mobile phone use, managing stress, avoiding smoking, eating a balanced diet, and staying physically active.
Author
Dr. Ganesh Veerabhadraiah
HOD & Senior Neurosurgeon | Neurovascular Specialist