Recognizing Trigeminal Neuralgia – When Everyday Activities Become a Nightmare
“Doctor, even talking hurts…”
A 36-year-old woman visited our clinic with a complaint that had completely changed her life.
For nearly four years, she had been living with severe episodes of facial pain. It was not an ordinary toothache, headache, or sinus pain. She described it as an intense electric shock shooting across the right side of her face.
The attacks were sudden.
They lasted only a few seconds, but the pain was so severe that she dreaded the next episode.
The most heartbreaking part was that even normal daily activities had become impossible.
Simple actions such as:
- Talking
- Smiling
- Brushing teeth
- Washing her face
- Swallowing food
- Drinking water
- A gentle breeze touching her face
could trigger excruciating pain.
Every morning she woke up wondering whether the pain would strike again.
Gradually, fear became a part of her daily life.
Instead of enjoying family conversations, she preferred silence.
Instead of eating comfortably, she ate cautiously.
Instead of stepping outside, she feared the wind.
She was no longer living normally.
She was merely trying to avoid pain.
The Pain That People Cannot Imagine
Most people assume facial pain is related to the teeth.
Many patients undergo repeated dental procedures.
Some even have healthy teeth removed.
Others receive treatments for sinusitis, migraine, or jaw disorders.
Unfortunately, the real cause often remains undiagnosed.
Trigeminal neuralgia is one of the most painful neurological disorders known.
The pain is often described as:
- Electric shock
- Lightning strike
- Knife stabbing
- Burning current
- Sudden explosion inside the face
Patients frequently say,
“Doctor, I would rather tolerate any other pain than this.”
The attacks are unpredictable.
Some patients experience a few episodes every day.
Others may experience hundreds of attacks.
Each attack may last only seconds, but the anticipation of the next attack creates enormous psychological stress.
Why Is It Called the “Suicide Disease”?
Historically, trigeminal neuralgia earned the unfortunate nickname “the suicide disease.”
This term emerged many decades ago because, before effective treatments were available, some patients became so overwhelmed by relentless, unbearable pain that they lost hope.
Today, fortunately, this condition is highly treatable.
With modern medications and advanced microsurgical techniques, most patients can achieve significant relief and return to normal life.
The term remains a reminder of how devastating the pain can be—not a prediction of what patients should expect today.
Understanding the Trigeminal Nerve
The trigeminal nerve is the fifth cranial nerve.
It is responsible for sensation over almost the entire face.
It has three major branches:
- Forehead and eye region
- Cheek and upper jaw
- Lower jaw
When this nerve is irritated, pain can occur anywhere along these regions.
Patients may experience pain in only one division or in multiple areas simultaneously.
In this patient’s case, the pain involved almost the entire right side of the face—from the forehead to the cheek and jaw.
Common Symptoms of Trigeminal Neuralgia
Patients often report:
- Sudden electric shock-like facial pain
- Severe stabbing pain
- Pain lasting seconds to minutes
- Repeated attacks
- Triggering while talking
- Pain during chewing
- Pain while swallowing
- Pain while brushing teeth
- Pain while shaving or applying makeup
- Pain triggered by washing the face
- Pain due to cold wind
- Fear of touching the face
Unlike migraine, patients usually have no nausea or visual symptoms.
Unlike dental infections, there may be no swelling or fever.
Unlike stroke, there is usually no weakness.
The pain itself is the major problem.
Years of Medicines
Our patient had already consulted multiple doctors.
She had been prescribed three different medications commonly used for trigeminal neuralgia.
Initially, they reduced the attacks.
However, over time:
- The pain gradually returned.
- The attacks became more frequent.
- Higher doses became necessary.
- Side effects started affecting her daily life.
Many patients taking long-term medications develop:
- Drowsiness
- Fatigue
- Dizziness
- Difficulty concentrating
- Memory disturbances
- Reduced work efficiency
Although medicines remain the first line of treatment, they do not permanently cure the underlying cause when a blood vessel is compressing the nerve.
Looking Beyond the Symptoms
When facial pain persists despite appropriate medications, it becomes essential to identify the underlying cause.
A detailed neurological examination was performed.
The pattern of pain strongly suggested trigeminal neuralgia.
The next important step was imaging.
A specialized MRI scan was advised to evaluate the trigeminal nerve and surrounding blood vessels.
The scan revealed the answer.
A small arterial loop arising from the brainstem was closely compressing the trigeminal nerve exactly where it exits the brainstem.
Every heartbeat caused repeated pulsatile compression of the nerve.
Over months and years, this continuous irritation had damaged the protective covering of the nerve, leading to abnormal pain signals.
Instead of transmitting normal facial sensation, the nerve began producing severe electric shock-like pain.
The diagnosis was now clear.
The challenge was deciding the best treatment.
Should medications continue?
Or should the compression itself be relieved?
That decision changed her life.
In Part 2, we discuss how modern microsurgery—Microvascular Decompression (MVD)—removed the cause of the pain rather than simply controlling the symptoms, allowing this young woman to become pain-free within a day after surgery.
The second part continues the patient’s journey through diagnosis, surgery, and recovery.
Patient Success Story: Trigeminal Neuralgia Relief After MVD Surgery
From Unbearable Electric Shock Pain to a Pain-Free Smile
Microvascular Decompression – Treating the Root Cause of Trigeminal Neuralgia
After carefully reviewing the MRI scan, the diagnosis became clear.
The trigeminal nerve was being compressed by a small arterial loop near its origin from the brainstem.
Every heartbeat caused the artery to repeatedly pulsate against the nerve.
Instead of merely treating the symptoms, our goal was to remove the cause of the pain.
After discussing all available options—including continued medical therapy, minimally invasive procedures, and surgery—the patient elected to undergo Microvascular Decompression (MVD).
What Is Microvascular Decompression?
Microvascular decompression is considered the most physiological surgical treatment for classical trigeminal neuralgia caused by vascular compression.
Unlike procedures that intentionally damage the nerve to reduce pain, MVD preserves the trigeminal nerve while relieving the pressure exerted by the offending blood vessel.
This approach aims to maintain normal facial sensation while eliminating pain.
Planning the Surgery
High-resolution MRI helped identify the neurovascular conflict.
Routine investigations were completed, and the patient was counseled about the procedure, expected outcomes, and possible risks.
The objective was simple:
Separate the artery from the nerve permanently.
The Operation
Under general anesthesia, the patient was positioned carefully.
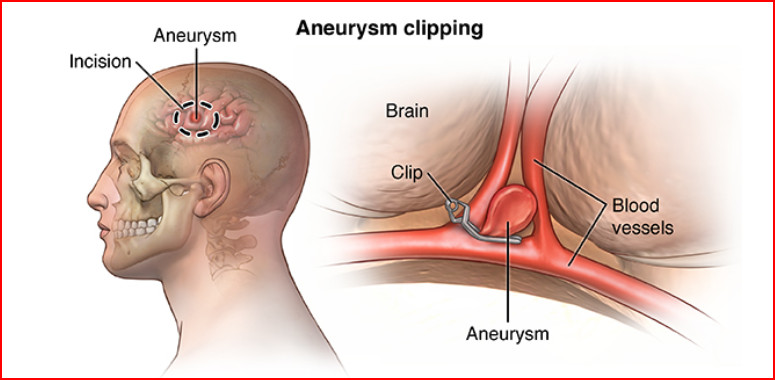
A small incision was made behind the ear.
A keyhole retrosigmoid craniotomy, roughly the size of a coin, provided access to the cerebellopontine angle.
Using the operating microscope and meticulous microsurgical techniques, the cerebellum was gently relaxed without unnecessary pressure.
The trigeminal nerve was identified as it emerged from the brainstem.
Careful inspection confirmed what the MRI had suggested.
A vascular loop was compressing the nerve at its root entry zone.
This is the most common site responsible for classical trigeminal neuralgia.
The artery was delicately mobilized away from the nerve while preserving its blood flow and surrounding structures.
A small Teflon felt patch was then placed between the artery and the nerve.
This tiny cushion prevents the artery from repeatedly striking the nerve with each heartbeat.
Once decompression was complete, the nerve was free from pulsatile compression.
Hemostasis was ensured, the dura was closed in a watertight fashion, the bone flap was replaced or reconstructed as appropriate, and the wound was closed in layers.
The procedure addressed the underlying cause rather than simply masking the pain.
Recovery
The following morning brought wonderful news.
The patient smiled and said something she had not been able to say comfortably for years.
She had no facial pain.
She could speak.
She could swallow.
She could smile.
She could gently touch her face without fear.
The electric shock-like attacks had disappeared.
Seeing this transformation is one of the most rewarding aspects of treating trigeminal neuralgia.
Why Does MVD Work So Well?
The trigeminal nerve is similar to an electrical cable.
Repeated compression damages its insulating layer.
This causes abnormal electrical discharges that the brain interprets as severe pain.
By separating the artery from the nerve, these abnormal discharges gradually stop.
In many patients, pain relief is immediate.
Others experience progressive improvement over days to weeks.
Long-term pain relief after successful MVD is excellent in appropriately selected patients.
Who Is a Good Candidate?
Microvascular decompression may be considered in patients who:
- Have classical trigeminal neuralgia.
- Show vascular compression on MRI.
- Continue to experience severe pain despite medications.
- Cannot tolerate medication side effects.
- Are medically fit for surgery.
- Desire durable pain relief while preserving facial sensation.
Not every patient requires surgery, and treatment should always be individualized.
Life After Surgery
Following successful decompression, many patients gradually reduce and discontinue pain medications under medical supervision.
They often regain confidence to:
- Eat comfortably
- Laugh freely
- Brush their teeth normally
- Return to work
- Resume social activities
- Sleep peacefully
- Live without constantly fearing the next attack
For someone who has lived with severe pain for years, these ordinary activities become extraordinary victories.
An Important Message
Persistent facial pain should never be ignored.
If you experience recurrent electric shock-like pain triggered by talking, chewing, brushing your teeth, or touching your face, seek evaluation by a neurologist or neurosurgeon.
Early diagnosis can prevent years of unnecessary suffering.
Modern imaging can identify the underlying cause, and effective treatments—from medications to advanced microsurgery—are available.
No one should have to live with relentless facial pain when help exists.
A Story of Hope
This young woman’s journey reminds us that even one of the most severe pain disorders can often be successfully treated with timely diagnosis, careful evaluation, and the appropriate intervention.
Her courage, patience, and trust in treatment helped her reclaim a normal life.
Today, she has returned home smiling, pain-free, and looking forward to a future no longer controlled by fear.
As neurosurgeons, moments like these reinforce why we strive for precision, compassion, and excellence in patient care. Every successful operation is more than a technical achievement it is an opportunity to restore dignity, confidence, and quality of life.
Frequently Asked Questions
1. What are the early symptoms of trigeminal neuralgia?
Early symptoms of trigeminal neuralgia include sudden, electric shock-like pain on one side of the face. The pain may be triggered by everyday activities such as talking, chewing, brushing your teeth, washing your face, or even a light breeze. These episodes typically last a few seconds but can occur repeatedly throughout the day.
2. What is the main cause of trigeminal neuralgia?
The most common cause of trigeminal neuralgia is a blood vessel pressing against the trigeminal nerve near the brainstem. This constant pressure damages the nerve’s protective covering, causing severe facial pain. In some cases, multiple sclerosis or tumors may also contribute to the condition.
3. How is trigeminal neuralgia diagnosed?
Trigeminal neuralgia is diagnosed through a detailed medical history, neurological examination, and MRI scan. An MRI helps identify whether a blood vessel is compressing the trigeminal nerve or if another underlying condition is causing the facial pain.
4. When is Microvascular Decompression (MVD) surgery recommended?
Microvascular Decompression (MVD) is usually recommended for patients with classical trigeminal neuralgia whose pain is not adequately controlled with medication or who experience significant medication side effects. It is most effective when MRI confirms blood vessel compression of the trigeminal nerve.
5. Is Microvascular Decompression surgery a permanent solution for trigeminal neuralgia?
Microvascular Decompression is considered one of the most effective long-term treatments for trigeminal neuralgia caused by vascular compression. By relieving pressure on the nerve rather than damaging it, MVD can provide lasting pain relief while preserving normal facial sensation.
6. Can trigeminal neuralgia be mistaken for a dental problem?
Yes. Many patients initially believe they have a tooth or gum problem because the pain affects the jaw or face. However, if dental treatments do not relieve the pain and it feels like an electric shock triggered by routine activities, trigeminal neuralgia should be evaluated by a neurologist or neurosurgeon.
7. What happens if trigeminal neuralgia is left untreated?
Without treatment, trigeminal neuralgia attacks may become more frequent and severe. Patients often avoid eating, speaking, smiling, or brushing their teeth due to fear of triggering pain, significantly affecting their quality of life.
8. Which doctor should I consult for trigeminal neuralgia?
If you have recurring electric shock-like facial pain, consult an experienced neurologist or neurosurgeon. Early diagnosis and timely treatment can help identify the underlying cause and provide effective pain relief before symptoms worsen.


 ಸುರಕ್ಷಿತ ಆಯ್ಕೆ ಮಾಡುವ ದಾರಿ:
ಸುರಕ್ಷಿತ ಆಯ್ಕೆ ಮಾಡುವ ದಾರಿ: