Brain tumours may be cancerous (malignant )or non-cancerous (benign). Almost 1 million cases occur in a year in India. Exact Cause is usually not known. Brain tumour can arise primarily in brain called Primary brain tumour and secondarily can arise from other part of the body and spread to brain called secondaries or metastatic brain tumours.
1. Benign – slow growing, not cancerous and won’t spread to surrounding structures
2. Malignant – fast growing, cancerous and spread to surrounding structures. May reoccur after the treatment.
Most common brain tumours – Meningiomas, Gliomas, Pituitary adenomas, Acoustic schwannomas.
I) Primary brain tumours –
1. Meningiomas – Arise from meninges
2. Gliomas – Arise from brain and spinal cord.- astrocytomas, glioblastomas, ependymomas, oligoastrocytomas,and oligodendrogliomas.
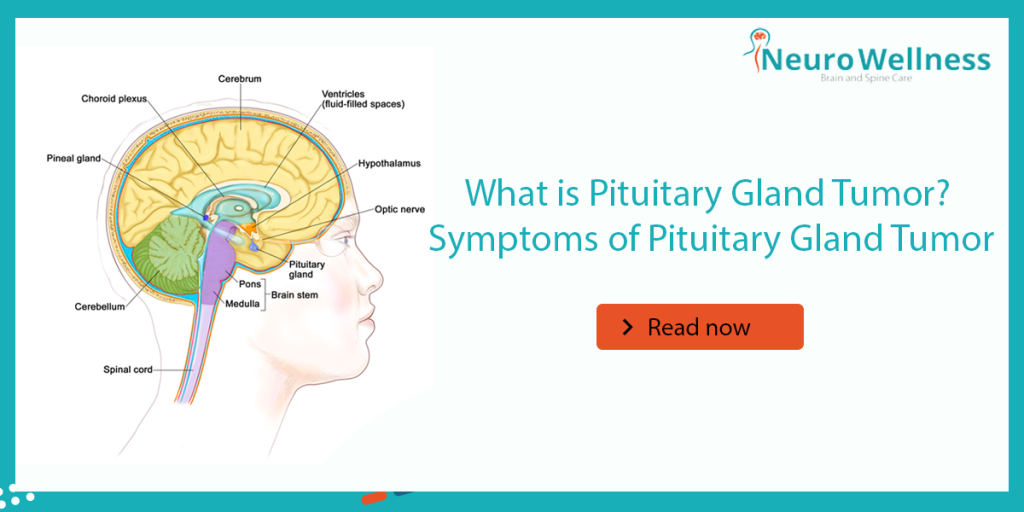
3. Pituitary adenomas
4. Acoustic schwannomas
5.Craniophyryngiomas-non cancerous
6. Medulloblastomas- common in children and behind brain and spreads in cerebrospinal spinal fluid.
7. PNET – Primitive neuroectodemal tumour, starts in embryonic cells of brain. These can occur anywhere in brain.
There are 4 grades
• Grade 1
• Grade 2
• Grade 3
• Grade 4
Lower the grade is least malignant(usually no contrast enhancement), grade 4 is highly malignant(contrast enhances).
II) Secondaries(metastatic) –
Secondary (metastatic) brain tumours are tumours that result from cancer that starts elsewhere in your body and then spreads (metastasizes) to brain. Secondary brain tumours most often occur in people who have a history of cancer. But in rare cases, a metastatic brain tumour may be the first sign of cancer that began elsewhere in your body.
In adults, secondary brain tumours are far more common than are primary brain tumuors.
Any cancer can spread to the brain, but common types include:
• Breast cancer
• Colon cancer
• Kidney cancer
• Lung cancer
• Melanoma
• Prostate
• Thyroid
• Gynecological tumours
Risk factors are
• Neurofibromatosis
• Ionising radiation
• Epstein Barr virus
• History of cancer in the family
• Exposure to vinyl chloride
All headaches are not due to brain tumours, all tumours may not produce headaches.
• Headaches in the morning
• Extreem nausea
• Headache relieved by vomiting
• Vision problems
• Seizures
• Repeated episodes of headache Symptoms depending on location of tumour-behaviour disturbance, ataxia
Management – Brain tumours are diagnosed by
• CT Scan-screen the brain most of the time.
• MRI SCAN – to know the exact location and spread.
• MR Spectroscopy – to know the nature.
• PET scan – to know the secondaries.
• ANGIOGRAM – to see the brain vessels
• Biopsy from the tumour.
Survival
Median survival
1. Low grade astrocytoma is 5 years or more
2. Glioblastoma – 1 year
3. Anapalastic astrocytoma – 3 years
Lower grade can be converted into higher grade
Treatment –
1. Surgery – Surgery is the usual first treatment for most brain tumours. Neuroradio-imaging, earlier diagnosis, systematic planning, preoperative, anaesthetic management, Neuro microscopes and surgical micro instruments, it is possible to remove significant amounts of brain tumour through relatively safely. For most cases, Brain Tumor Treatment in Bangalore is often successful and a full recovery is possible, although there’s sometimes a small chance the tumour can reoccur. Regular follow-up is advised to monitor.
The advent of PET CT, IGRT(image guided radiation therapy) and Gamma knife surgery(stereotactic radio surgery) is revolutionizing the treatment of various problems in the brain, including benign brain tumours in eloquent locations, like the motor cortex, basal ganglia, brain stem or near the optic nerve. Howsoever, all Brain tumours do not require operation and many are treatable with radiation or chemotherapy or Gamma Knife.
1. Radio surgery
2. Gamma knife
3. Chemotherapy
Advances in tumour surgery – which has made brain surgery safe
1. CUSA(Cavitron ultrasonic surgical aspiration)
2.Neuronavigation(minimally invasive)
3. Awake craniotomy(to resect tumour accurately
4. Interventional MRI(real time surgery)
1. Neuroendoscopy
2. Pre-operative embolisation(endovascular to minimise bleeding)
3. Sterotaxy
Rehabilitation –
• Physiotherapy
• Speech therapy
• Occupation therapy

Dr. Ganesh Veerabhadraiah
Consultant – Neurosurgeon, Neurointerventional Surgery, Spine Surgeon (Neuro)
23+ Years Experience Overall (17+ years as Neuro Specialist)
Available for Consultation: Jayanagar 9th Block & Kauvery Hospital, Electronic City
FAQs
1) What are the early symptoms of a brain tumor?
Persistent headaches, morning nausea or vomiting, seizures, vision or speech changes, and weakness or numbness in limbs. Symptoms vary by tumor location and size.
2) Are all brain tumors cancerous?
No. Some are benign (non-cancerous) and grow slowly; others are malignant (cancerous) and may grow faster. Both can cause symptoms and require evaluation.
3) When should I see a neurosurgeon for suspected brain tumor symptoms?
If headaches are new/persistent, seizures occur, or you notice progressive neurological changes (vision, speech, balance, weakness), seek prompt specialist evaluation.
4) How are brain tumors diagnosed?
Clinical exam plus imaging—typically MRI (preferred) or CT. Additional tests may include MR spectroscopy, perfusion studies, or biopsy for a definitive diagnosis.
5) What are common treatment options for brain tumors?
Options include surgery, radiosurgery, radiotherapy, chemotherapy, targeted or immunotherapy, and supportive care. Plans are individualized by a multidisciplinary team.
6) What affects recovery and prognosis?
Tumor type/grade, location, molecular markers, extent of safe removal, and patient factors (age, overall health). Early detection generally improves outcomes.
About Author
Dr. Ganesh Veerabhadraiah
Dr. Ganesh Veerabhadraiah, leading neurosurgeon and neurologist in Bangalore, has over 20 years of expertise in managing back pain, migraines, headaches, neuro disorders, and spine problems. His clinical excellence and patient-first approach make him one of the most trusted neuro doctors in Bangalore.
At Neurowellness Brain & Spine Clinic in Jayanagar and Kavery Hospital Electronic City, Dr. Ganesh provides comprehensive treatments ranging from minimally invasive spine surgery to advanced neurological care. As a respected back pain specialist and migraine doctor, he continues to deliver reliable outcomes for patients.
👉 Connect with Dr. Ganesh on LinkedIn